Multicounty Outbreak of Salmonella Agbeni Linked to Ice in a Cooler at a County Fair — Illinois, August 2024
Investigation and Results
Case Definitions
CDC’s definition of a confirmed case of salmonellosis as a clinically compatible illness (e.g., diarrhea, abdominal pain, nausea, and sometimes vomiting) with laboratory isolation of a Salmonella species from a clinical specimen (1) was applied to all persons who became ill and had attended the fair. A probable case was defined as a clinically compatible illness epidemiologically linked to a confirmed case (e.g., shared exposure at the fair) but without culture confirmation, including a positive nonculture diagnostic method such as polymerase chain reaction testing without subsequent culture confirmation (1). This investigation was conducted as part of a public health response activity and was determined to be public health practice, not human subjects research; therefore, it was not subject to Institutional Review Board review.
Patient Characteristics
Seven laboratory-confirmed cases of salmonellosis caused by S. Agbeni were identified through the National Electronic Disease Surveillance System among residents of five Illinois counties who had attended the fair (Table). In addition, six probable cases in close contacts of persons with laboratory-confirmed infection were also identified through patient interviews; these persons reported milder signs and symptoms (nausea and diarrhea) and did not seek testing or medical care. All 13 patients were aged 23–53 years. Ten cases occurred in men and three in women. Two of the six probable cases occurred in spouses of persons with confirmed cases; these persons reported similar, but milder, gastrointestinal symptoms.
Potential Sources of Exposure
Food, inadequate hand hygiene, and portable toilet use. Initial hypotheses regarding infection source focused on foodborne illness linked to vendor-prepared meals or possible contamination from the communal portable toilets. All 13 persons who became ill were interviewed using a foodborne illness questionnaire provided by the Illinois Department of Public Health. Although nine persons who became ill reported that they had purchased and eaten food from one or more of six different vendors on different days, four patients had not eaten at the fair at all. Two patients reported that they cleaned their hands using their own personal hand sanitizer, and 10 patients reported that they did not wash their hands. Four patients reported never having used the portable toilets. None of the persons who became ill sat in the grandstand or worked in the livestock barns. However, all 13 persons who became ill reported 1) spending time in the infield area and 2) drinking canned beer from the beer tent. No illnesses were identified among persons who did not access the beer tent.
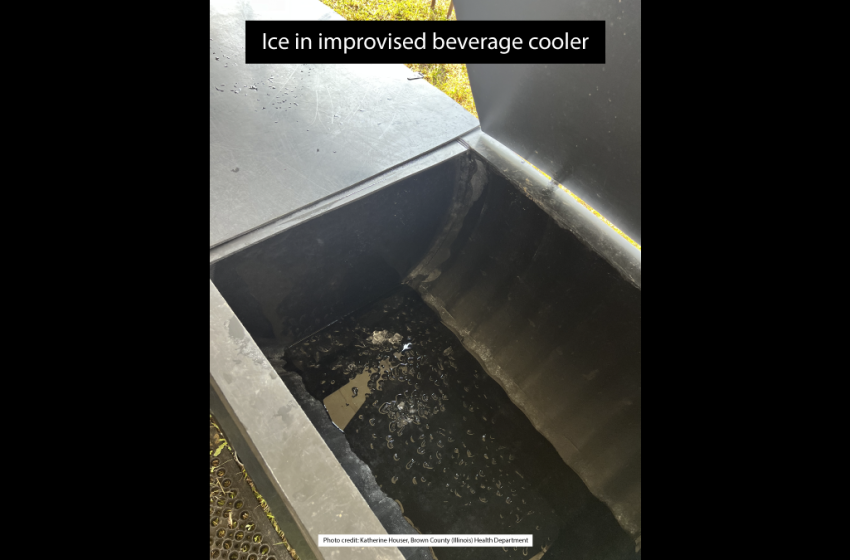
Ice in the beer cooler. BCHD staff members conducted interviews with persons who had worked at the beer tent during the fair to ascertain how the cooler and beer cans were handled. Fair organizers reported that the large improvised cooler in the beer tent consisted of a 10-ft length of non–food-grade corrugated black plastic farm drainage tile with four internal compartments. The cooler was only meant to contain ice and cans of beer. The ice for the fair was provided by a single local company and produced from a municipal water supply, and all fair vendors had access to the same ice for use in their vendor stalls. The cooler was rinsed out with a hose once at the beginning of the week. The cooler was not rinsed again and was never cleaned with soap, and no means for monitoring the cooler’s internal temperature was available. Staff members handled the ice and cans with their bare hands. Handwashing stations were not available inside the beer tent. Cans were kept submerged in ice, and the melted ice was replenished daily. The cooler was designed to drain through a single spigot; however, standing water was reported, suggesting incomplete drainage. Different staff members worked at the beer tent each night, including two persons who later received test results positive for salmonellosis; both reported drinking beer at the beer tent and were the only staff members who reported illness. The standing water in the cooler was not reported until after the fair had concluded and was not available for testing, nor was the cooler itself. No standardized cleaning or sanitization procedures for the cooler were reported.
The BCHD food inspector confirmed with BCHD communicable disease investigative staff members that ice can become contaminated if handled or stored improperly, consistent with the Illinois Food Code (77 Ill. Adm. Code 750.100: definition of contaminated food, and 750.330: protection from contamination after receiving), which recognizes ice as food and subject to contamination risks (2). A 2013–2023 systematic review documented contamination of food ice with enteric bacteria and viruses (e.g., coliforms and Escherichia coli, Staphylococcus aureus, Vibrio spp., and norovirus) and fungi, most often linked to inadequate ice-machine sanitation and handling; contamination was more common in ice produced on-site in food businesses than in industrially manufactured ice, supporting ice as a plausible contributor to cross-contamination and gastrointestinal outbreaks (3).
Patient Interviews
Some interviewed attendees were hesitant to provide details because they did not want to implicate other members of their community. One patient with laboratory-confirmed salmonellosis reported observing leftover food stored overnight in the ice cooler on August 1. Fair board members stated that this practice was not permitted. Because the investigation was retrospective, the report could not be independently verified; however, unauthorized food storage in ice used for beverages represents a potential mechanism for cross-contamination.
Measures to Identify Additional Cases
Because the community was small and close-knit, health department staff members attempted to identify additional cases by contacting personal acquaintances and monitoring social media posts and photos to identify persons who had attended the fair or visited potential areas of exposure. During August 12–21, health department staff members contacted fair board members and persons who they knew had attended the fair to ascertain whether these persons had visited the beer tent and whether they or persons they knew had become ill. No additional cases were identified.
Artificial Intelligence Hypothesis Generation
Drinking beer from the fair’s beer tent was the only common exposure reported among all persons who became ill. Because the investigation began >1 week after the fair concluded, the ice and water were no longer available for testing, nor was the cooler. In the absence of other common food or environmental exposures, contamination of the ice used for beer storage was considered a plausible source for the outbreak. A generative artificial intelligence (AI) large language model (ChatGPT 4.0, OpenAI; 2024) was used to generate hypotheses of other possible sources of exposure by reviewing exposure patterns and identifying potential transmission pathways, supplementing the ongoing traditional epidemiologic investigation. No other common exposure sources were identified. On August 21, information regarding which days each fair attendee became ill, the vendors from whom they purchased food, what each person ate and drank, and whether the patients were in the infield or the grandstand was entered into the AI model, followed by a series of questions.
The first question entered into the AI model was, “Will S. Agbeni grow in an improperly drained cooler?” ChatGPT responded that S. Abegni could grow in a cooler under conditions that are favorable to Salmonella growth, including standing meltwater combined with hot summer days and lack of sanitation. The second question was, “Are any other sources, other than ice, likely if only canned beverages and no foods were available at this location?” The AI response indicated that Salmonella-contaminated meltwater contacting the exterior of beverage cans, followed by hand-to-mouth transfer of bacteria, was a plausible route of exposure. The third question was, “What is the likelihood that these infections occurred through contaminated ice rather than another exposure?” The AI response compared alternative hypotheses and indicated that, given the environmental conditions described and that no common food was identified, ice contamination was the most consistent explanation. The fourth question was, “Why would some persons become ill whereas others remained well?” The AI response suggested that variation in exposure dose, differences in how persons handled the cans, and fluctuations in the water temperature throughout the day might account for the distribution of illnesses. The fifth question was, “What examples of similar outbreaks have been documented in scientific literature?” The AI response identified studies in which contaminated ice or beverages stored in ice were linked to outbreaks of enteric illnesses (3–5). The final question entered into the AI model was, “What is the probability of a Salmonella outbreak linked to contaminated ice?” The AI response did not provide a definitive number but emphasized that such outbreaks are well-documented in the literature and represent a credible and likely source in this setting. The AI response further suggested that ice contamination is often an overlooked transmission vector, which might explain why precise probabilities were difficult to establish despite recurring evidence of its role in enteric outbreaks.
First Appeared on
Source link

