National analysis of cancer mortality and proximity to nuclear power plants in the United States
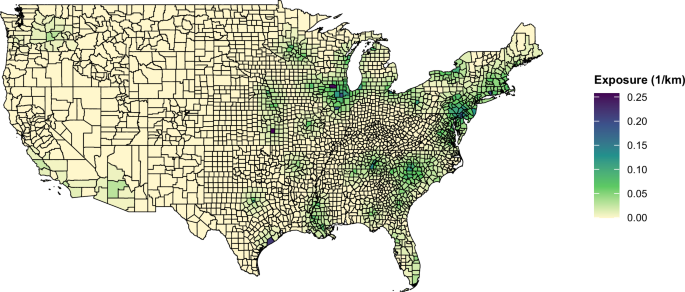
We assessed the relationship between long-term proximity to nuclear power plants and cancer mortality using a spatially resolved, inverse-distance weighted proximity metric that captures cumulative contributions from multiple plants within 200 km of each U.S. county center. We observed positive associations between proximity and cancer mortality, with stronger effects in older age groups (Fig. 3). The highest attributable cancer mortality burden was observed among individuals aged 65–74 and 75–84, particularly among males (Table 1), reflecting both greater vulnerability in older populations and latency patterns typical of environmentally related cancers. Overall, cancer mortality among individuals aged 65 and older, associated with proximity to nuclear power plants, averaged 4266 deaths per year (95% CI: 3000–9122) between 2000 and 2018.
To contextualize these findings, we compared our results to estimates of mortality associated with another major energy source—coal. A recent study estimated that total all-cause mortality attributable to coal-fired power plant emissions averaged 20,909 deaths per year (95% CI: 19,091–22,727) over 22 years (1999–2020)26. While this is not a direct comparison—since our study examines cancer-caused mortality, whereas the coal study estimates all-cause mortality—our findings represent approximately 20% of the total coal-attributable deaths in their study. This comparison underscores the magnitude of cancer burden within the broader landscape of energy-related health risks.
Ionizing radiation is a well-established carcinogen, with extensive epidemiologic evidence linking radiation exposure to increased cancer risk6,7,27. Some of the strongest evidence comes from studies of nuclear disasters, where high-dose radiation exposure has been consistently associated with increased cancer incidence.
The Japanese atomic bomb survivor Life Span Study first identified excess leukemia deaths, which were observed were first observed about 2 years after the bombing and continued to be seen for the next 25 years after the disaster. Over time, elevated risks of solid cancers emerged, including cancers of the esophagus, stomach, colon, liver, lung, and urinary bladder, as well as female breast, brain, thyroid, and non-melanoma skin cancers. These cancers were first observed 10 years after the bombing and persisted throughout the lifetime of the cohort28,29,30,31.
Epidemiologic findings from Ukraine following the Chernobyl disaster in 1986 have been inconsistent. A study investigating solid tumor trends 30 years after the disaster found increased incidences of colon, rectal, kidney, thyroid, breast (in women), and prostate (in men) cancers, although decreases in lung and stomach cancers were also reported32. In contrast, another study suggested that post-Chernobyl cancer incidence trends largely mirrored pre-disaster trends, implying no significant excess risk due to radiation exposure33.
Studies investigating the effects of nuclear power plants on cancer incidence in surrounding communities have reported mixed findings. A study in France examining proximity to nuclear power plants and 12 cancer types found an excess incidence of bladder cancer in both males and females20. Similarly, a study in Spain investigating the Trillo and Zorita power plants reported that the risk of all cancers increased linearly with proximity to the plants17. However, other large national studies, including those conducted in the United States8,9,25, the United Kingdom15, and Canada1, have found no consistent associations between residential proximity to nuclear power plants and overall or site-specific cancer incidence or mortality.
A German study focusing on pediatric cancers found a statistically significant risk ratio (RR) of 2.2 for leukemia and an RR of 1.6 for solid tumors among children under five years old living within 5 km of nuclear power plants compared to those living further away34.
The relationship between nuclear power plants and cancer risk has also been examined in South Korea, Canada, and China, with conflicting results. A study in South Korea found elevated cancer incidence in populations near a nuclear power plant, including thyroid cancer (HR: 3.38 in females, 1.74 in males), female breast cancer (HR: 2.24), and radiation-related cancers (HR: 1.59 in males, 1.77 in females). In contrast, the study reported no increased risk for radiation-insensitive cancers (HR: 0.59 in males, 0.98 in females)35.
Studies in Canada and China found no clear association between proximity to nuclear power plants and cancer incidence. A study in Ontario, Canada, reported no consistent pattern for all cancers combined or for specific cancers such as thyroid, lung, breast, stomach, colon, bladder, brain, liver, leukemia, and non-Hodgkin lymphoma among populations living within 25 km of three nuclear plants1. Similarly, a study in China on the Qinshan Nuclear Power Plant found no increased risk for all cancers, leukemia, or thyroid cancers36.
While differences in nuclear power plant technology and emission controls may contribute to variation across studies, much of the observed heterogeneity in findings likely stems from differences in exposure assessment methods, study designs, statistical power, and outcome definitions. Many previous studies relied on binary proximity cutoffs rather than incorporating cumulative proximity from multiple plants, which may have introduced measurement error by oversimplifying exposure levels in these ecological studies. In contrast, our study uses a continuous, inverse-distance weighted nuclear power plants proximity metric, allowing for a more refined assessment of long-term exposure gradients.
Additionally, studies that focus on single plants or small geographic areas may have limited statistical power, particularly when assessing rare cancers. These studies may lack sufficient case numbers to detect associations, whereas larger-scale national studies,like ours, have the advantage of higher statistical power and the ability to capture regional nuclear power plants proximity variability.
Our study has several limitations. First, our nuclear power plant proximity exposure assumes equal contribution from all nuclear power plants within 200 km and does not include direct radiation measurements (dosimetry). Second, we analyzed all cancer types combined, even though different malignancies have varying latency periods and radiation sensitivities. Third, our analysis was done at the county (FIPS) level because that is the resolution at which the CDC provides cancer mortality data. This ecological design does not capture individual-level exposure or outcomes and therefore limits causal inference. Moreover, our exposure metric reflects geographic proximity rather than actual radiation exposure experienced by individuals. Fourth, we did not analyze childhood cancers. These outcomes were rare in our dataset, and stratification by age group, sex, county, and year resulted in sparse data and unstable estimates. Proper evaluation of childhood cancer risk would require different modeling approaches tailored to rare outcomes. Fifth, we used a standard formula for calculating the attributable fraction (AF), which assumes a causal relationship between exposure and outcome and does not account for potential unmeasured confounding or exposure misclassification. Finally, our analysis does not incorporate residential histories, and exposure assignment was based on the geographic centroid of each county. While this limits temporal precision compared to individual-level cohort studies, there is no evidence that residential mobility is systematically related to proximity to nuclear plants. As such, any exposure measurement error is likely non-differential, which would bias results toward the null. Our study spans nearly two decades, and we also assume long-term residence stability throughout this period. Despite these limitations, to our knowledge, this is the only national study in the U.S. to examine nuclear power plant proximity and cancer mortality using a continuous proximity metric. Unlike prior studies that focused on single plants, small geographic areas or relied on fixed distance cutoffs to assign binary exposures, our approach provides a comprehensive and a continuous assessment of nuclear power plants proximity across the entire country, capturing the cumulative impact of multiple facilities over nearly two decades and enhancing statistical power to detect potential associations. Additionally, we used a continuous, inverse-distance weighted proximity metric instead of categorical proximity-based definitions, allowing for a more nuanced and comprehensive exposure assessment.
We also utilized a nationally representative, long-term cancer mortality dataset from the CDC, ensuring high data completeness and broad geographic coverage. The inclusion of a full 19 years of cancer mortality data (2000–2018) and a 10-year average nuclear power plants proximity window allows for a robust temporal assessment of long-term proximity effects.
We found that U.S. counties located closer to operational nuclear power plants experienced higher cancer mortality rates, with the strongest associations observed in older adults, particularly among males aged 65–74 and females aged 55–64. These results indicate a spatial association between residential proximity to nuclear power plants and cancer mortality. This study focused exclusively on cancer mortality and did not examine neurological, cardiovascular, or other potential health outcomes associated with nuclear facilities. While current evidence remains insufficient to draw definitive causal conclusions regarding cancer risks among populations living near nuclear plants, our findings highlight an important area for future investigation. Understanding the potential long-term health implications of nuclear power generation is particularly important given the renewed interest in nuclear energy as a low-carbon solution, emphasizing the importance of addressing these potentially substantial but overlooked risks to public health.
First Appeared on
Source link

